Concern about breast cancer risk remains one of the most important reasons many menopausal women hesitate to consider hormone therapy (also labeled as hormone replacement therapy, or HRT). This concern largely traces back to the Women’s Health Initiative (WHI) study published in the early 2000s, which profoundly influenced how hormone therapy was viewed by both patients and doctors.(1)(2)
Since that time, a growing body of research has clarified how breast cancer risk varies by hormone formulation, timing of initiation, and individual health factors. Current clinical guidance from The Menopause Society reflects updated evidence on individualized assessment and hormone-specific risk.(3)
The following article provides an updated, evidence-based review of what the latest science shows about HRT and breast cancer risk, drawing on findings from 10 peer-reviewed studies to place earlier concerns in a clearer context.
Why HRT and Breast Cancer Became a Source of Fear
Hormone therapy remains the most effective treatment for menopause-related symptoms, but its clinical use has been shaped by how the WHI findings were initially interpreted. The 2002 WHI publication found a slight but important increase in breast cancer risk among postmenopausal women using combined estrogen-progestin therapy. These findings suggested a link between certain forms of HRT and an increased risk of breast cancer, leading to widespread concern.(2)(4)(5)
Recently, the FDA updated its stance on menopause hormone therapy, but that does not mean it’s risk-free. In reality, HT still involves some risk, which is why full assessment and personalized care are necessary. Newer studies show that breast cancer risk is not uniform but individualized. It varies based on who uses HRT, when it is started, the type of hormones used, how they are delivered, for how long, and individual risk profile. These distinctions are essential for making informed decisions based on current evidence and avoiding conclusions based on a single study or outdated assumptions.(2)(4)(5)
The WHI Study: What It Found and What Was Missed
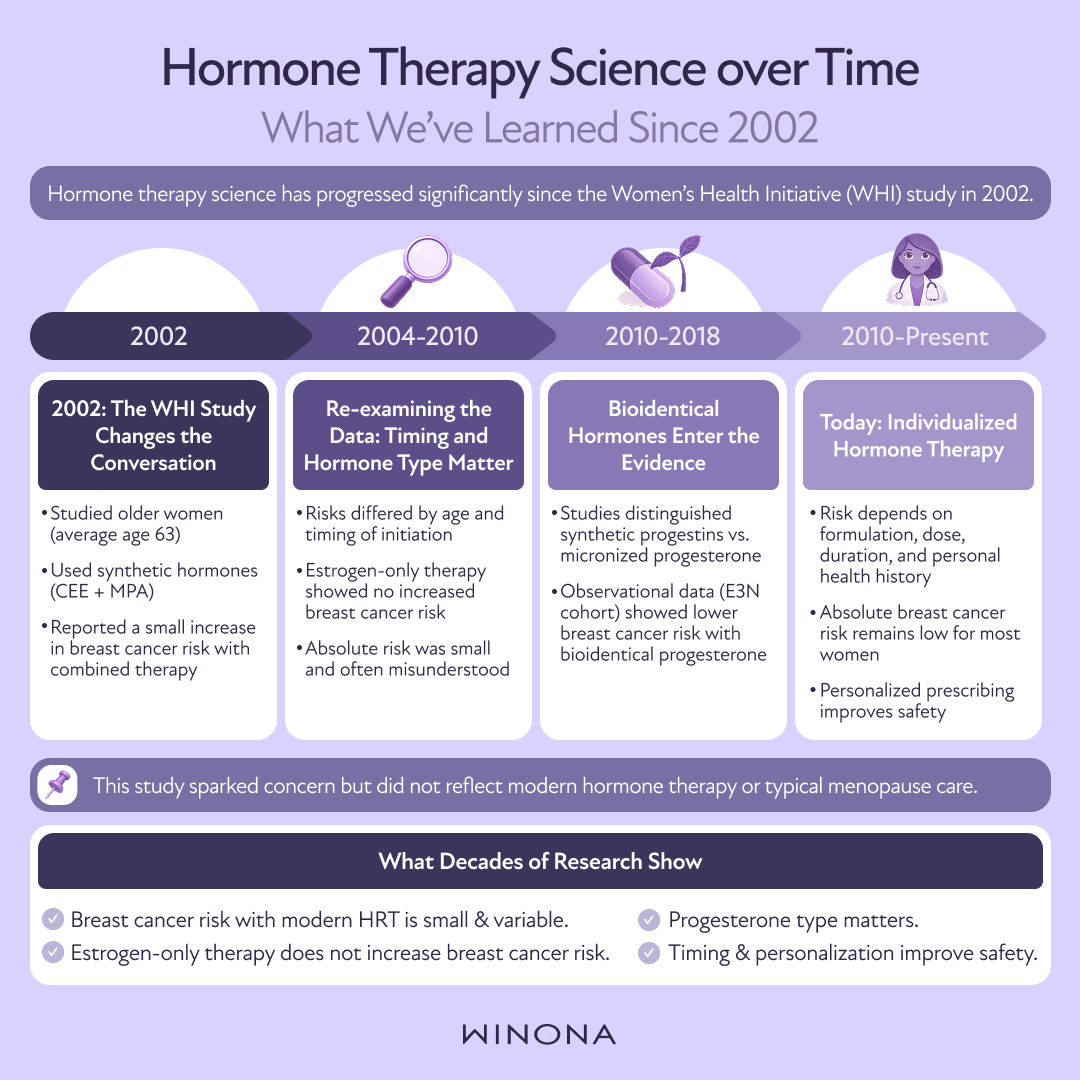
The WHI was a large, randomized trial designed to examine the long-term health effects of hormone therapy. The combined therapy branch studied conjugated equine estrogen (CEE) with medroxyprogesterone acetate (MPA), both older-generation synthetic hormones.(2)(5)(6)
Key Findings
A small increase in breast cancer risk was observed with combined estrogen–progestin therapy.
No increased risk was seen in women using estrogen-only therapy after hysterectomy.
The increased risk was not equally applicable to all forms of hormone therapy.
Important Limitations
Subsequent analyses have revealed several limitations of the WHI findings, making it important to recognize that the study’s results have often been misinterpreted.(2)
Several factors limit how broadly these findings apply today:(5)(6)(7)(8)(9)(10)(11)
Population Specificity: The study focused on women with an average age of 63, whose risk profiles are different from those of women just entering menopause. Many of the participants began hormone therapy years after menopause — this differs from women who start HRT closer to menopause, where risks may vary.
Delivery Methods: The study did not factor in the risk differences between oral (systemic) therapy and skin-applied (transdermal) therapy.
Formulations: The study did not distinguish between synthetic and bioidentical hormones, which carry different risk profiles. It exclusively examined synthetic hormones — CEE and MPA — which have distinct risks compared to bioidentical hormones.
Absolute vs. Relative Risk: The reported risk increase was relative, translating to a modest absolute risk for most women. For example, the increase equated to about eight cases of breast cancer per 10,000 women annually.
These distinctions help explain why WHI findings were widely misinterpreted and why modern guidance has evolved.
Not All HRT Is the Same: Breast Cancer Risk by Therapy Type
HRT involves the administration of estrogen, usually combined with progesterone, to alleviate menopausal symptoms such as hot flashes, night sweats, and vaginal dryness. There are two main types of HRT.
Combined Estrogen–Progesterone Therapy
The American Cancer Society notes that for women with an intact uterus, progesterone is required to protect against the risk of endometrial cancer. This is also where a small increase in breast cancer risk has been observed.(6)(7)(12)
For women with a uterus, progesterone is necessary to reduce the higher relative risk of uterine cancer caused by estrogen, even though it may slightly increase the risk of breast cancer.
Progesterone protects the endometrium by balancing out estrogen, thus lowering the risk of uterine cancer. However, it also stimulates breast tissue growth, possibly leading to abnormal changes.
Risk appears time- and dose-dependent, increasing more noticeably after five or more years of continuous use.
Risk declines after discontinuation.
Outcomes vary significantly based on the type of progesterone used and individual factors.
Estrogen-Only Therapy
Primarily used in women who have had a hysterectomy (removal of the uterus), estrogen-only therapy has the most favorable breast cancer risk profile.(5)(8)(13)
Estrogen, on its own, stimulates the lining of the uterus to grow, which can raise the risk of endometrial cancer in individuals with an intact uterus.
Women who have had a hysterectomy can safely use estrogen-only therapy, as they do not need the protective effects of progesterone, thus eliminating progesterone-related breast tissue stimulation.
WHI follow-up data showed no increase in breast cancer risk with estrogen-only therapy.
Some analyses suggest a slightly reduced risk compared with no hormone therapy.
The Progestin Factor: Why Progesterone Type Matters
Not all progesterone is the same. The WHI used MPA, a synthetic progestin that behaves differently in breast tissue than bioidentical progesterone.
What Newer Data Suggests
Micronized progesterone, which is chemically identical to endogenous progesterone, appears to have a more favorable breast safety profile.(8)(9)
Large observational studies, including those from the E3N cohort, found that estradiol combined with micronized progesterone was not associated with increased breast cancer risk, unlike combinations using synthetic progestins.(8)(9)
Higher doses or continuous daily progestin — not progesterone — appear to carry more risk than sequential or intermittent use.(9)
These distinctions are central to modern hormone therapy practice.
Putting Risk in Perspective: Absolute vs. Relative Risk
Breast cancer risk is often reported using relative risk, which can make changes seem larger than they truly are.(5)(9)(10)
For example:
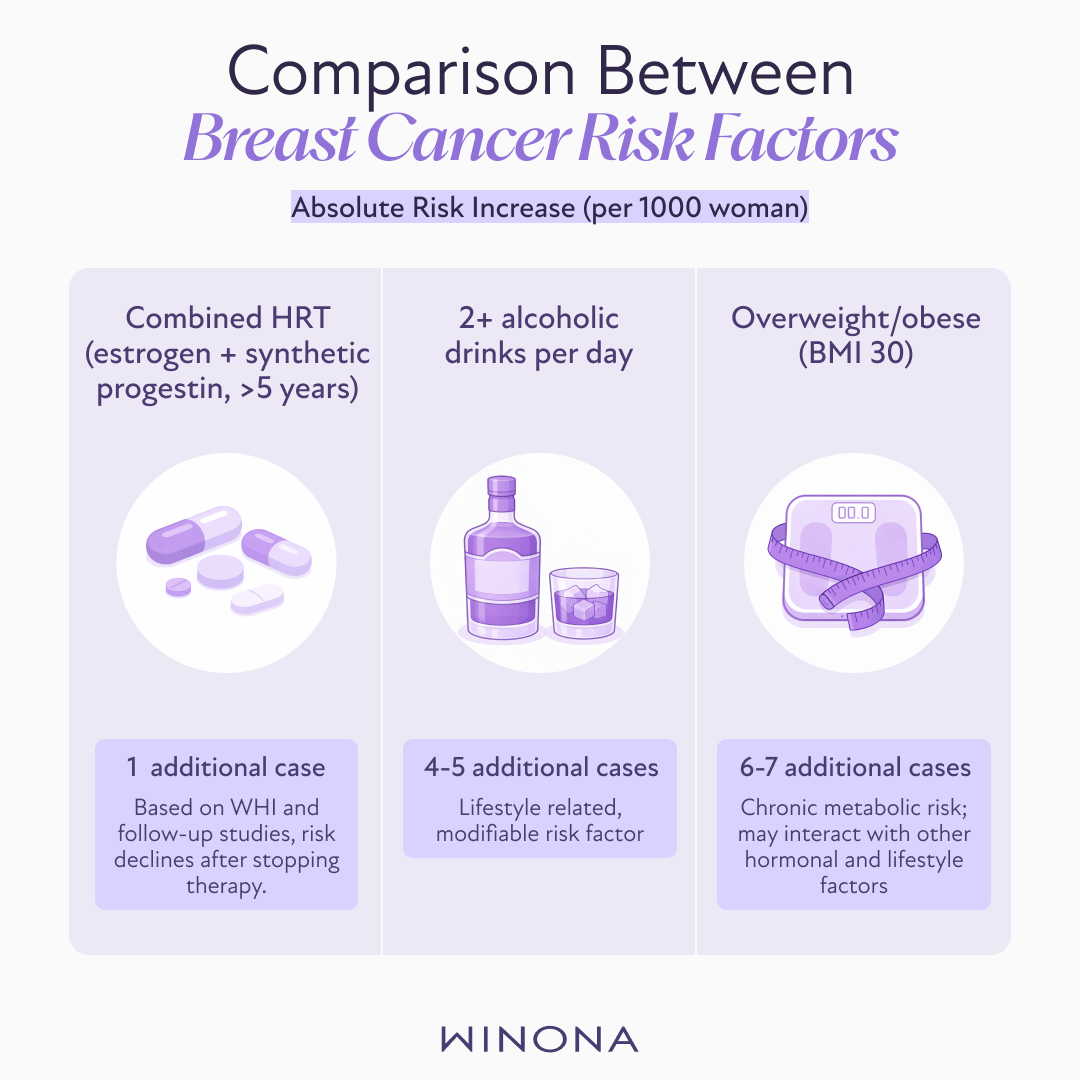
Say one out of 1,000 women is expected to develop breast cancer this year, and that number increases to two out of 1,000 next year, the relative increase is 100%. That sounds dramatic, but in absolute terms, it means only one additional case per 1,000 women.
Looking at risk this way helps clarify the real-world impact. For many HRT regimens, the absolute increase in breast cancer risk is small.(5)(9)(10)
In fact, it’s often lower than the risk linked to other established risk factors, such as the following:
Alcohol use
Obesity
Physical inactivity
Late age at first pregnancy
This is why risk framing is essential for informed, balanced decision-making around HT.
Delivery Method and Breast Cancer Risk
How hormones are delivered also matters.(11)
Transdermal estradiol (patches, gels, sprays) bypasses first-pass liver metabolism.
This route avoids stimulation of pro-inflammatory proteins linked to clotting and metabolic effects.
Emerging evidence suggests that transdermal delivery may contribute to a lower overall risk profile compared with oral formulations.
Weighing Benefits Against Risk
For appropriately selected women, hormone therapy offers well-documented benefits:(4)(5)(6)(7)(8)(10)(14)
Reliable relief from vasomotor symptoms
Preservation of bone density and fracture prevention
Improved sleep quality and physical well-being
Favorable cardiovascular markers when initiated near menopause onset
Favorable cognitive function markers (emerging research)
Risk is influenced by individual health history, genetics, timing, formulation, and duration — not by hormone therapy alone. For most women, the benefits of bioidentical hormones — when administered appropriately — outweigh potential risks.
Importantly, women should not hesitate to discuss their options with physicians who understand the nuances of hormone therapy.
Strategies to Minimize Breast Cancer Risk with HRT
The American Cancer Society points out that for women considering HRT, several strategies can help reduce breast cancer risk:(4)(6)
Using the lowest effective dose for the shortest duration necessary
Opting for bioidentical estradiol and micronized progesterone, when appropriate
Considering transdermal delivery
Integrating lifestyle measures that independently reduce breast cancer risk
Reassessing therapy regularly
Maintaining routine breast screening, mammograms, and follow-up
Considerations for HRT Use
Modern guidelines advocate for an individualized approach to HRT, weighing risks and benefits based on personal health history, symptom severity, and preferences.(4)(5)(6)(14)
Who May Benefit Most:
Women under 60 or within 10 years of menopause onset, experiencing significant symptoms
Women at risk of osteoporosis or fractures
Who Should Be Cautious:
Women with a history of breast cancer or other hormone-sensitive cancers
Women who carry genetic mutations that increase breast cancer risk (i.e., BRCA 1 and 2 gene carriers)
Those at high risk of cardiovascular disease or thromboembolism

HRT After Breast Cancer
Systemic hormone therapy is generally avoided in individuals with a history of breast cancer. However, local vaginal estrogen therapy is considered safe for treating genitourinary symptoms.(5)(13)
Key features of local vaginal estrogen therapy include the following:
Delivers low-dose estrogen directly to vaginal tissues
Minimal systemic absorption
No evidence of increased recurrence risk in clinical studies
Clinical evidence confirms that local estrogen therapy does not raise recurrence risk, making it a viable option for breast cancer survivors seeking relief from genitourinary symptoms.
A Personalized Approach Remains Essential
Hormone therapy remains the most effective treatment for menopause-related symptoms, offering substantial benefits for quality of life and long-term health when appropriately administered. Breast cancer risk with HRT is not uniform. It varies based on hormone type, formulation, delivery method, timing, and individual health factors. Modern evidence supports moving beyond one-size-fits-all conclusions toward personalized risk assessment guided by current science.(4)
The legacy of the WHI underscores the importance of context — not avoidance — in hormone therapy decisions. When evaluated carefully, HRT remains a valuable, evidence-based option for many women navigating menopause.